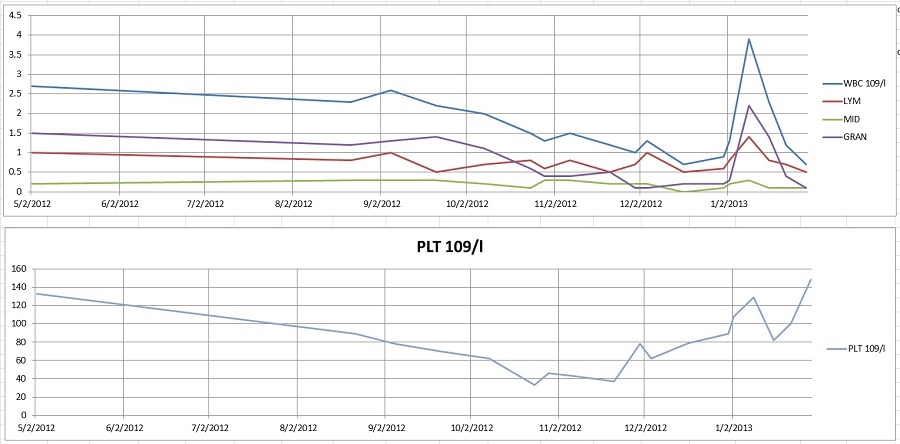

Haven’t been posting much the last month, because my blood counts were in a slump and I didn’t want to worry relatives who might be reading this. But now that horse is out of the barn door, since a bone marrow biopsy this week showed that, five months or so after my transplant, my cancer has come back. I won’t know until Thursday what the docs at Johns Hopkins are recommending for me.
Obviously, this sucks. It is really not what I wanted, and I was just starting to think that this whole crazy transplant vs. cancer thing might really be working out in my case.
I feel a weird sense of clarity, kind of like what I felt when I got diagnosed with this cancer last year. Partly it’s that I clearly need to focus on short-term goals: eating (I lost a few pounds in the last month of suspense, and keeping my weight up is important), staying connected with people, and being careful to avoid germs, and any risk of hitting my head while my platelets are so low.
Partly, though, it’s because I woke up Friday morning with the following song lyric running through my head:
In the shadows, frightened, we deny you, hiding, locking all our doors
But when you find us, you remind us–
You say, “All I have is yours.”
It is a good song (“Won Our Hearts”), and people should check out the album, by Chris Hoke/Tierra Nueva, on iTunes. Sometimes the recording quality is a little homespun, but that is because Chris is busy working on life-changing Bible studies with imprisoned gang members.
To be honest, at this particular moment I’d rather have more of a Proverbs/Psalms kind of vibe, with God healing my body and giving me long life here on earth and (in my case, adopted) children. And that could still happen–possibly through medicine or, as always, if God wills it. I’m certainly not giving up on either. But this song is what I get right now, so I’m sticking to it.

Raspberries with melted fair-trade bittersweet chocolate on the side.
I’m also taking this time to enjoy fresh raspberries (miraculously still available at the farmer’s market today though I didn’t get there till noon), not to mention showering without any tubes coming out of my body. Because everyone should enjoy those things.
…
All blog content copyright © 2012-2014 E. Palmberg. Guaranteed 100% brave and freaking noble.